


Click Above for Our Rumble Version / Click Below for Our Substack Version
jermwarfare with Summary, Commentary & Full Transcript by the Art of Liberty Foundation’s Etienne de la Boetie2
Jerm Warfare Interviews Dr. Denis Rancourt on 31 Million Deaths from Vax & Government Policies During “The Covid”
We usually reserve this Substack for our own research and writing but occassionally an interview or story comes along that is so important that we use our platform to ensure it receives the maximum amount of attention. This is one of those cases. In this interview award-winning South African political cartoonist and talk show host Jeremy “Jerm” Nell interviews world-class academic Dr. Denis Rancourt (h-index 41 & i10 index of 91) on his latest paper, Spatiotemporal variation of excess all-cause mortality in the world (125 countries) during the Covid period 2020-2023 regarding socio economic factors and public-health and medical interventions showing an estimated 31 million dead from the Covid “vaccines” and the government’s Covid policies. This supports our own investigations into”The Covid” as a eugenics operation: See Solving Covid – The Covid 19 Eugenics, Vaccine/Drug Scam Timeline at and its companion article: The Covid 19 Suspects and Their Ties to Eugenics and Population Control/Reduction
This analysis of global all-cause mortality during the COVID-19 era (2020-2023) suggests that there was no true pandemic based on mortality data from 125 countries. The study found an excess mortality rate significantly lower than historical pandemics like the 1918 Spanish Flu. Rancourt argues that the excess deaths were likely due to factors such as the COVID-19 vaccines, lockdown-induced stress, and certain government mandated medical interventions rather than a viral outbreak.
Dr. Rancourt breaks down the evidence for the majority of “Covid” deaths not attributable to the “vaccine” being misdiagnosed bacterial pneumonia on page 259 in their paper.
“To the degree that COVID-19 death assignation represents a serious respiratory condition at death, and given the intricate weekly temporal matching of the reported COVID-19 mortality and excess all-cause mortality for up to 3 years in the USA data, this represents strong evidence that respiratory infections were dominantly (virtually entirely) associated with excess all-cause mortality. Rancourt et al. (2021a) showed this in detail, into 2021 (their Figures 34a through 34i). They also pointed out that more than half of the deaths assigned as COVID-19 deaths could include life-threatening co-occurring bacterial pneumonia, according to CDC tabulations of death certificates, and that prescriptions of antibiotics were significantly reduced in the same period. Rancourt et al (2021a) fervently concluded:
“Finally, our examination of plausible mechanisms for the exceptionally large COVID-era mortality in the USA, given all our empirical observations, leads us to postulate that COVID-19 may largely be misdiagnosed bacterial pneumonia (using a faulty PCR test: Borger et al., 2021; and see Ginsburg and Klugman, 2020), that correctly assigned bacterial pneumonia itself largely goes untreated, while antibiotics (and Ivermectin) are withdrawn, in circumstances where large populations of vulnerable and susceptible residents have suppressed immune systems from chronic psychological stress induced by (“COVID response”) largescale socio-economic disruption, and that the USA has, in the COVIDera, thus recreated the conditions that produced the horrendous bacterial pneumonia epidemic of 1918 (Morens et al., 2008) (Chien et al., 2009) (Sheng et al., 2011).”
Here is a summary of the main points from the interview with a complete transcript to follow:
Global Analysis: Denis Rancourt’s study analyzed all-cause mortality data across 125 countries during the COVID-19 era (2020-2023).
Pandemic Skepticism: He argues that the data does not support the narrative of a global pandemic, as the excess mortality was not consistent with a pandemic scenario.
Alternative Causes: Rancourt suggests that excess deaths were more likely due to factors like the COVID-19 vaccines, lockdown-related stress, harmful medical practices (Remdesivir, ventilators, isolation, denial of antibiotics, etc.) and misdiagnosed bacterial pneumonia from faulty PCR test rather than the “virus” itself.
Comparison to Historical Pandemics: The study compares mortality rates to historical pandemics, particularly the 1918 Spanish Flu, which had significantly higher death rates.
Critique of Public Health Measures: Rancourt criticizes the public health response, claiming it caused more harm than the virus.
For more details, you can read the full conversation [here](https://jermwarfare.com/conversations/denis-rancourt-on-global-all-cause-mortality-of-the-entire-covid-era).

Introduction and Background:
– The interview begins with Denis Rancourt, a scientist who has been researching COVID-19 since the onset of the pandemic, discussing his views on the nature of the pandemic and the excess mortality observed during this period. He challenges the mainstream narrative by arguing that the excess mortality was not caused by a viral pandemic but by the responses to it.
Initial Findings and Publications:
– Rancourt’s first significant paper, published on June 2, 2020, posited that the peaks in excess mortality coincided with the announcement of the pandemic but were not caused by a viral spread. Instead, he attributed these peaks to aggressive medical treatments (Ventilators, Isolation, etc.) and mismanagement in hospitals, especially in hotspots like New York, France, and northern Italy.
– He points out that a virus does not wait for a political announcement to start killing people, suggesting that the synchronous mortality peaks around the world made no sense if the cause was viral.
Research Focus and Challenges:
– Rancourt and his team have since written 21 large reports on COVID-19, covering a range of topics from theoretical epidemiology to critiques of public health measures like masking. His work, especially the review showing the ineffectiveness of masks, gained significant attention, leading to censorship on platforms like ResearchGate.
– Despite being marginalized in mainstream scientific circles, Rancourt’s research has found a home in alternative media and has influenced public discourse on COVID-19.
Recent Major Study:
– Rancourt’s latest and most extensive study, Spatiotemporal variation of excess all-cause mortality in the world (125 countries) during the Covid period 2020-2023 regarding socio economic factors and public-health and medical interventions published in July 2024, examines excess mortality data from 125 countries. This 521-page paper, which includes over 600 figures and detailed statistical analyses, argues that the excess mortality observed during the COVID period was not due to a viral respiratory pandemic but to the measures taken in response to the pandemic, such as lockdowns, medical interventions, and vaccine rollouts.
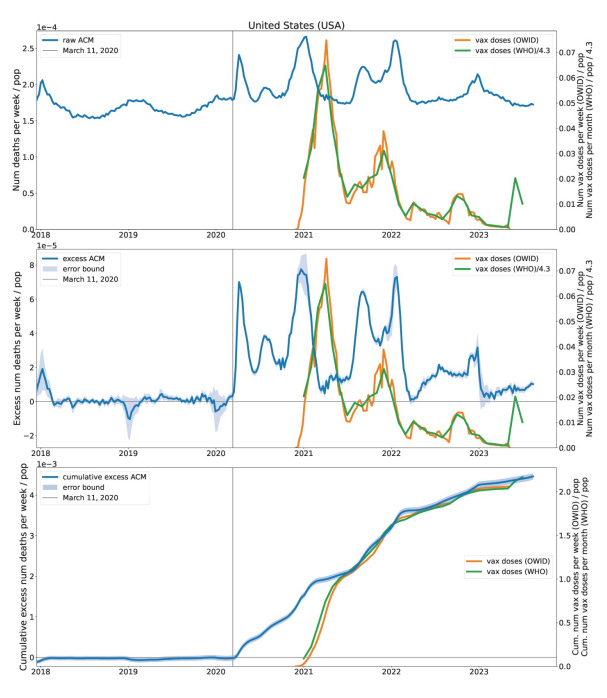
– The study found no significant excess mortality in any country until after the pandemic was declared by the World Health Organization on March 11, 2020. This observation challenges the idea that a viral pandemic was the primary cause of the global mortality increase.
Methodology:
– The study used “all-cause mortality” data, which Rancourt emphasizes is reliable and less susceptible to bias compared to other data types. This data tracks the total number of deaths, making it a robust metric for understanding mortality trends.
– The analysis included modeling historic mortality trends (starting from 2015) to project what mortality would have looked like without the pandemic. The differences between these projections and actual observed mortality were attributed to excess mortality.
Key Findings:
– Excess Mortality Estimates: The study estimates that 31 million excess deaths occurred globally during the COVID period, with about 17 million of these deaths linked to vaccine rollouts.
– Correlation with Poverty: The research found a strong correlation between excess mortality and poverty, particularly in the United States.
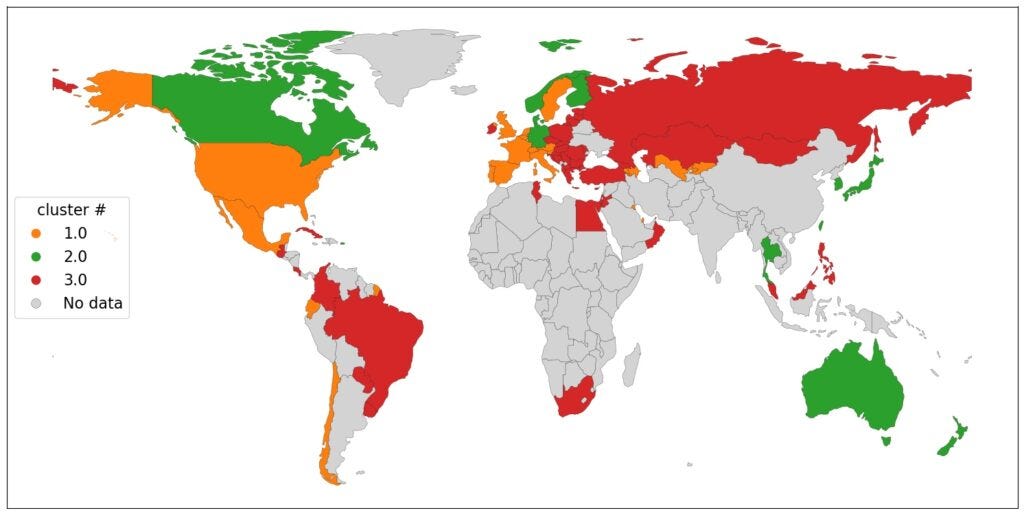
– Cluster Analysis: The study identified three main clusters of countries based on their excess mortality patterns:
– Cluster 1: Russia, Eastern Europe, and Northern Asia.
– Cluster 2: Europe and parts of North America.
– Cluster 3: Countries with low excess mortality until vaccination began, including Australia, Japan, and Canada.
Hypotheses and Interpretations:
– Primary Causes of Death:
1. Aggressive Medical Treatments: Includes the use of ventilators and denial of standard treatments, such as antibiotics for bacterial infections.
2. Biological Stress: Caused by lockdowns, isolation, loss of work, and other stress-inducing measures.
3. Vaccinations: The study links vaccine rollouts to spikes in excess mortality, particularly among the elderly and those who received multiple doses.
– Vaccination Effects: Rancourt hypothesizes that vaccines may cause direct toxicity, over-immune reactions, or immune suppression, all of which could lead to increased mortality.
Critique of the Scientific Establishment:
– Rancourt criticizes the current scientific environment, where he feels that researchers are reluctant to challenge the mainstream narrative on COVID-19 and vaccines. He argues that adverse effects of vaccines are underreported and that there is a broader ideological agenda at play.
– He suggests that the pandemic response was more of a military operation than a public health initiative, aimed at testing population control mechanisms.
Geopolitical Context:
– Rancourt views the COVID-19 pandemic and the global response as part of a broader geopolitical strategy, particularly by the United States, to maintain control and counter the rising influence of China and Russia.
– He warns of an ongoing class war in the U.S. and predicts further global instability as the U.S. faces economic decline. He stresses the importance of resistance against these global forces, particularly through the cohesion of nations opposed to U.S. dominance.
Conclusion:
– Rancourt concludes that if the pandemic had not been declared, there would have been no significant excess mortality. The deaths that occurred were primarily due to the aggressive and stress-inducing measures taken in response to the declared pandemic, not the virus itself.
Key Talking Points:
– The excess mortality during the COVID period was not due to a viral pandemic but to the responses to it, including medical treatments, lockdowns, and vaccines.
– The study estimates 31 million excess deaths globally, with 17 million linked to vaccine rollouts.
– Strong correlations were found between excess mortality and poverty, and different patterns of mortality were observed across different country clusters.
– The vaccines may have caused mortality through direct toxicity, immune overreaction, or immune suppression.
– The pandemic response is seen as a military operation aimed at testing and implementing population control measures.
– The broader geopolitical context, including U.S. strategies to counter China and Russia, plays a crucial role in understanding the pandemic and its aftermath.
Raw transcript

Rancourt: My pleasure.
Jerm: Every time you and I speak, the podcast goes berserk because you always have such interesting information to share, and I’m guessing that’s why we’re talking again. Let’s ease into it this time. Let’s talk about how you got here firstly to this particular paper. Well,
Rancourt: I’ve been working on, the science related to COVID ever since the very beginning. The very first paper I wrote in which I made some pretty bold statements, was back on the, it was published on the 2nd of June, 2020. It was about the fact that these huge mortality peaks, excess mortality peaks that were coincident with the announcement of the pandemic had nothing to do with an actual viral spreading pandemic. That it was entirely to do with how people were being assaulted and mistreated in hospitals and by treat, very aggressive treatments in hotspots like New York and certain hospitals in France and so on, and northern Italy. And so, I said, look, this is all about how you’re assaulting people. It has nothing to do with the pandemic. A virus does not wait for political announcement in order to decide to start killing people in certain places in the world.
Rancourt: And when there are peaks like this that cannot be synchronous, around the world, you know, so I pointed out that there, there is, this made no sense, and that this was a massive assault against people. That was way back then. And, you know, we’ve written 21 large reports about covid signs and reviews about the science, and, and that includes theoretical papers. Some were published in good scientific journals, peer reviewed the ones that were not too, radical in the eyes of the establishment, where, where we basically criticized how they were doing theoretical e epidemiology, things like that. And, you know, everything from, the nonsense of masking and the, the science behind it and everything, I was the first to make a big review of, of scientific articles about masking and how every single careful clinical trial showed that it was of no use whatsoever in terms of preventing an infection.
Rancourt: So we did that right off the start, and that got so many views, that they, they, cut me off on, on ResearchGate. And, it, it, it got everybody very excited that, that people would be interested in hearing about this. So I’ve just been going on, big report after big report, and we’ve added, many, researchers who are collaborators. And so it’s led to deeper and deeper work. We created a nonprofit, corporation called Correlation Research in the Public Interest. We try to fund that with, with donations, and that’s, that multiplies our ability to do science and to get it out there. And so we’ve been just doing this constantly, and I think we’ve produced some very high quality work, and a lot of it has been noticed quite a lot to the point where it almost gets into the mainstream media, right.
Rancourt: But it gets into the, the big alternative venues. One of the things we, are famous for is having demonstrated that there’s an association in time between vaccine rollouts and large peaks in excess mortality. And we’ve been able to quantify how many deaths would be associated to vaccines in this way and so on. And we did more of that in this recent big paper and really confirmed that, that that had to be true yet again, now using 125 countries. Whereas before we’d only studied a couple of dozen countries. So we just keep, keep on marching. And this latest paper is our biggest one to date. And it’s, I think, the biggest study of its kind using excess, all cost mortality. It’s, 521 pages. It’s got more than 600 panels of figures. It’s got detailed explanations of everything and examination of all the correlations with social economic parameters, advanced statistical techniques applied to this data. And, it just came out on the 19th, of July. And, there was some immediate, media tension. So a lot of people noticed it on Substack and elsewhere. This is the first interview I do about it because, I promised that I would do this with you as soon as it came out, and so on. Just
Jerm: For clarity, Deni, somebody who knew that I was gonna chat to you, asked me to ask you, what do you classify as the start of Covid?
Rancourt: The announcement of a pandemic by the World Health Organization was the 11th of March, 2020. I would consider that the start of the Covid period. And then, in, I think it was the 5th of May, 2023, they announced that the, there was no longer a pandemic, an end to the pandemic. Right. Okay. So the paper that we just wrote covers that entire period and goes beyond it somewhat into 2023. And what’s important is to know from the all cause mortality around the world, all the hun, the more than a hundred countries that we studied, there was no excess mortality anywhere in any country, in any jurisdiction until they announced a pandemic. So the virus was waiting for the announcement, waiting behind the gate there to come out. And that in itself is, is a demonstration that this was not a viral respiratory pandemic.
Jerm: Also, just for clarity, because it’s been a few years now since you and I have been doing this series of interviews, your research into all cause modalities is particularly interesting because it’s one field of, of study that a lot of scientists have simply ignored. Just quickly as a summary, what is all-cause mortality?
Rancourt: The kind of data here is nations count their dead , they count deaths. They, they really good, they have statutory requirements. They set up institutions. They have a whole process with checks and balances where they count deaths, because it’s a very important thing for the nation to know is, how many people died when they die How old were they Where did they die All this kind of thing. deaths like births are very important to a nation, a a modern nation to plan things and so on, and to know if something special is happening and how to foresee how things are gonna evolve economically and otherwise in, in the human society. So that’s very important. So they do it very well, and they’ve been doing it for more than a hundred years in, in the Western countries. And so there’s really good data. It’s hard data in the sense it’s not amenable to manipulation.
Rancourt: You really just are counting the dead. So it’s not susceptible to bias regarding cause of death or anything. Whatever caused the person that died. They died, and they died on this day. And here we have the data, you know, it’s really good data in that sense. And it was ignored by the scientific establishment at the start of covid. It took a while before scientists started using it and talking about it and comparing it to what they call Covid death. So now there are more and more articles coming out that use all cause mortality data, but when I was doing it, there was virtually none. Death
Jerm: Is a death. You can’t really hide it. I mean, it’s something that you will invariably find out
Rancourt: If you’re set up to, to legally register it and that it’s an obligation, and that all the MDs and the professionals and the institutions are, are following the law and are doing this, then you’re gonna end up with some pretty good death statistics. And every time we’ve done checks and balances to see if the statistics are good in, in places where they are good, they, they’re, they’re excellent. I mean, there are a few weird things like, like in the uk there’s a day in the week where they don’t like to, or a day in the year rather, where they don’t like to register deaths. Maybe the, the people who who signify them, don’t like to go out that day. I forget what day of the year it was. might have been Christmas or something. And, so there’s a, a drop in the deaths, you know, that you see systematically every, every time that’s the uk there’s some little peculiarities here and there, but generally it’s incredibly high quality data.
Rancourt: Yes. So this latest paper came out on the 19th of July of this year, 2024. As I said, it’s a massive paper. It’s co-authored with, Joseph Hickey and Christian Ard, who is at the University of Quebec. And vie it’s the result of years of work. And now we’re looking at 125 countries. And so we’ve got this mortality by week or by month at least. That that was, that was a requirement, is that we have it by time and we need to have it over an extended period of time because we need to start before covid because we need to, kind of extrapolate and see what the historic trend would’ve been if there had not been covid. And so we do that mathematically. And then the difference between what, what is predicted if nothing special had happened and what is actually observed, that’s the excess all cause mortality.
Rancourt: And so we measure and quantify that excess all cause mortality. And the excess itself varies with time, because different things were happening at different times when they first were very aggressive, when they had, crazy protocols in certain jurisdictions when they rolled out this booster or that injection, when they put on this horrendous lockdown, they kept people at home. All these things coincide with, with, surges in all cost mortality. And you see it in this excess that we measure. So we can quantify all that, and then we can look for correlations between those quantified excess mortality in different time periods and social economic parameters, for example. So one of the big things that comes out whenever we, study this is there’s always a very strong correlation to poverty. So how many people are, are living in the nation under poverty We were the first to demonstrate this in, in really strong terms for the United States in, in a paper way back.
Rancourt: And we see this very, very clearly in this big paper. We apply something that’s called hierarchical cluster analysis. They’re very different mortality behaviors from country to country. And so we, we wanted to see if there was groups of countries that kind of behaved the same way. And we were able to identify three main clusters of countries that have the same kinds of patterns of all cause mortality. And so what we see is Russia and Eastern Europe and Northern Asia fall into the same cluster. And then, Europe and North America, some of North America, is another cluster. And then there’s this cluster that is very peculiar ’cause it’s very small, all cause mortality. And it only arises really when you start vaccinating. So that cluster contains Australia, Japan, Canada, few places like that. So you can see these clusters on a world map. You can then study the statistics on a per cluster basis, on a per country basis.
Rancourt: I mean, we did so many things. We really took a very thorough look at what was happening in the world. This, you know, the, the spatial temporal variation of excess mortality and its correlation to everything that we can know about that, where we can have data. And that’s the nature of this paper. And so we concluded a few things. Our big conclusions, I would say are what we think are the most likely hypotheses to interpret what we saw, right That that’s what it is. there’s some conclusions that are just hard numbers. It’s not interpretation. It’s actually a result. You know, like for example, 31 million people died in excess, excess mortality during the covid period projected in the world. Okay 31 million, yes. That’s the number that we get. And we have a, a, a very good quantification of that projected to the world from the 125 countries and testing if some of the big countries that were excluded had similar behaviors by, by looking at individual studies of those countries, we’re convinced that that’s very close to the real number.
Rancourt: So it’s much larger than what is thought to be COVID-19 deaths. And then of that 31 million, we estimate about 17 million deaths of those are associated with the vaccine rollouts. And we have presented, a lot of data and reasons and arguments as to why you must make this association with the vaccine rollouts. One of the strongest arguments that comes out is the temporal, synchronicity or association between rollouts and peaks in excess mortality. That is very, very evident in some jurisdictions. And in most jurisdictions, there’s, there’s correlations like that, and there’s peaks that are correlated. And so we see, for example, that this kind of death that’s associated with the vaccines is greater among the more elderly people. So it’s exponential in age, and it’s stronger, if you like. The correlation is stronger and the effect is bigger the further you are in the doses.
Rancourt: So for the first booster and second booster, as you go into more and more doses, the impact of the vaccination as seen in this association is stronger and stronger. So those are the kinds of things that we see, and we see it systematically in every country that we studied. We have very good numbers for this, vaccine dose fatality rate is what we call it. There’s a lot of variability, but still, this is what we, we believe is happening. The 31 million deaths is a hard number. And well, you have to project to the world, but the number we have for the 125 countries, that’s a hard number. It’s, it’s not disputable. the, the, the methods are right. The data is hard. And we’ve got the equivalent of 31 million deaths in the world when you project it. So what we do is we have 125 countries, and we can quantify in each one the total excess deaths that occurred during the Covid period.
Rancourt: We add all that up, and we get a certain number of, millions of deaths for the 125 countries. And then we say, well, we’ve got countries all around the world on every continent, poor and rich countries, every kind of country you can think of. So we think this is representative of what would’ve happened, given that everyone was responding to Covid in the, in these kinds of ways. Everybody had and developed VA and gave vaccines and everything. So how many deaths would there have been around the world So you project that, to the world, given the world population, and you get 31 million for the world. It’s a more accurate number than that. I forget the exact number. I think it’s 30.9 plus or minus 2 million. You know, this is all based on official all cause mortality data from the countries as they record it for themselves and communicate it to various agencies that want to collect it. It’s official data for those nations. That’s what we use.
Jerm: Take me through some of that, that methodology.
Rancourt: You typically have all cause mortality by week or by month, let’s say. So each week or each month, you know how many deaths occurred in the particular jurisdiction. So the jurisdiction can be the entire nation, or it could be a province or a state within the nation. but you, you, you do it by jurisdiction. So every week, let’s say you, you have the total number of deaths, but you know that from before Covid, we started our data in 2015, our examination. And so what you see, is in the Northern Hemisphere, there are ways before you get to Covid, there’s a seasonal variation of mortality, of excess mortality. That’s just a really well known epidemiological phenomenon in the northern hemisphere. It’s, the mortality is higher in there, in our winter, in the northern hemisphere, in the southern hemisphere, the mortality is seasonal also, but it’s higher in the winter of the southern hemisphere, which is our summer.
Rancourt: So it’s inverted. This is all really well known. Elderly people die more in the winter, and there’s a lot of hypotheses as to why that is. nothing really conclusive, but there’s some good, good ideas about why that happens. But it does. So that is the historic trend, this seasonal variation near the equator. There’s no seasonal variation. It’s a flat line. It’s very clear. So it’s very beautiful when you look at our data, because we have all these countries, you can actually see in the pre covid era, the seasonal variation in the, in the northern latitudes, the flat line on the equator, and then it’s inverted or shifted, if you like, phase shifted in the southern hemisphere where it’s in, it’s six months later that you have this maximum in mortality, you see So that’s the historic baseline before you get into covid. And what we do is we model that seasonal variation in a way that we develop that’s very clever, I think, which I won’t tell you the mathematical details, but we model that to be able to project it into the future.
Rancourt: So we projected into the future, into the CO period to see what mortality would’ve been like in the Covid period. And when you, when you look at our graphs, it’s very convincing because our modeling method matches before covid really, really well. And it looks like naturally that’s what would’ve happened. Okay And then we’ve got error propagation, we’ve got error bars on that and everything, but then the mortality in the covid period has these peaks that are above what would’ve been predicted. So when you take the difference between what we predict in this way and the actual mortality, that’s the excess mortality. So you’re getting the excess at every time interval at every week or at every month. And so you can plot what the excess mortality looks like per week. And so that is indeed a flat line until you announce the pandemic, then it can have a peak, or, or in many countries it can remain essentially a flat line until you roll out the vaccines.
Rancourt: And then you have a peak related to the rollout of the vaccine and so on. Every country is different because the different countries were doing different things. They were applying different medical protocols, they were locking down more or less aggressively. They were, vaccinating with different vaccines and sometimes at different times and more or less rapidly and all this kind of stuff. So whatever the countries were doing in terms of these various assaults is directly reflected in the mortality that results among fragile people to the degree that they have a lot of elderly, fragile people. And so that’s what the conclusion of our study is, is that there is a perfect understanding of these excess mortalities in terms of what was actually being done. One of the important results of our work, Jeremy, I have to tell you this. When you look at all this, you have to know that we’re not just analyzing data.
Rancourt: We’re also very knowledgeable about the theory of, let’s say viral respiratory spread. You know, the standard models, we’re very knowledgeable of that. We’ve written peer reviewed journal articles about the theory, so we know what the establishment would say, how this happens, and how the theory works. And so we know when we look at the data that it is incompatible with the notion of a viral respiratory disease spread. Yeah, pandemic. Yeah. Okay. So we basically disprove the hypothesis that there was a pandemic. And I wrote an essay about this, which you’ve read, which is entitled, Canada: There was No Pandemic. And I’ve explained all this, all the reasons why you have to conclude. There was no pandemic in the sense of a novel pathogen that was spreading in the way that they say it spreads. Okay So that’s one of the main results of this paper, is that it’s, it’s yet another, this time definitive in the sense that it’s 125 countries demonstration that the spatial and temporal variations disprove that hypothesis.
Rancourt: It should be abandoned. There was no pandemic. Now don’t forget, we’ve said this before in our past papers, none of the declared pandemics of the CDC since 1918 have given rise to any detectable excess. All cause mortality. And covid did have large detectable excess mortality. But the pattern is inconsistent with the theory of a pandemic. But the ones before where they were not applying these aggressive methods, they didn’t give rise to any excess mortality, irrespective of all the papers that were estimating the numbers of deaths and so on. We don’t see them. When you do a rigorous analysis of excess mortality in the way that I explained, you don’t see any signal from these pandemics. So there is no evidence in modern data that the CDC promoted pandemics are actually real. They actually occur as, as they propose. That’s one of the big results of our paper.
Rancourt: There are a lot of results. So I, I explained, that the vaccines are associated with death. I can explain later if you want, what the mechanisms of that association would be. Another big result of the paper, which is, an understanding that we’ve come to over years of study is the following. We’ve come to understand, therefore, that there are three big categories of primary causes of death during the covid period. Excess mortality, there’s three primary causes, but then there’s, beside the primary causes, there’s the observed proximal clinical conditions of the person who died, which is different than the primal cause of death. Okay So what I mean by that is, for example, let’s say you, you, you know how to suppress the immune system of a person, and you do it, and as a result, they develop an infection, either of their gut or their lungs or something.
Rancourt: You know, infections are historically have been the main killer always in humanity. It’s only in modern times that we’ve controlled infections by the conditions in which we live in and using antibiotics and so on. Okay So let’s say you suppress immune systems and, and a person gets an infection and then dies. What killed the person It’s whatever you did to suppress their immune system that killed them. That’s the primary cause. Whatever infection they end up getting is an observed clinical condition at death. But it’s not the primary cause of death. It’s not the driver of why they died early compared to what would’ve happened if you hadn’t done that. You see what I mean So we distinguish this primary cause of death from these associated conditions at death, and I’ll tell you what those associated, associated conditions are that we’ve discovered. But among the primary, causes of death, what we found are the following first aggressive medical treatment that would not normally be recommended and shouldn’t be recommended.
Rancourt: And that causes death. And that’s many different ventilators, huh Ventilators, yes. Mechanical ventilators, various kinds of drug protocols that were used, you name it. There, there were a lot of medical interventions, and I would include in that category of medical interventions, not giving medical treatment. Because normally when people get bacterial lung infections, they are treated appropriately with antibiotics. The, let’s say, expert pharmacist at the hospital does the usual tests, finds out that in this case, it’s mainly these three bacteria that are responsible. Therefore, the targeted drugs are these ones in this amount, and therefore you treat them and they get better. None of that was being done during covid. They stopped prescribing antibiotics, even though they admit that there was massive amounts of bacterial lung infections. The CDCs own records as more than half of the people who had respiratory conditions, which were assigned to COVID-19, had co bacterial pneumonia, which was not treated, generally speaking.
Rancourt: So, denial of medical treatment is a primary cause of death in the sense that normally people do get lung infections, and normally in the last few years we’ve been treating them, and then you stop treating them. Well, that’s a primary cause of death, okay So I would include denial of treatment as part of that as well. So that’s one big primary cause of death. The other one is everything you do that causes biological stress, which includes psychological stress, enormous stress on the person. So that includes taking away their work, their activity, isolating them, making them locked down, all of these things, all these horrible things. You know, there was a, a recent study that we cite in our paper that showed that if you take mice and you just confine their movements for a couple hours, there are dramatic effects on their health as a direct result of the biological stress that’s induced by simply preventing them from moving, okay
Rancourt: For a short time. So biological stress is massively important in terms of health, and it depresses your immune system, therefore, you know, it, it, it’s a real killer. All the measures and everything that we’re doing for the whole structure of the society and the economy is, is another primary cause of death. And the third one is, the medical interventions known as COVID-19 vaccination. So those are the three primary causes of deaths that we hypothesize on the basis of all our data. The other thing that’s really interesting that we discovered is if you look at the excess mortality of function of time, it matches exactly in modern countries with good data. How many respiratory conditions are associated with death as a function of time In other words, the great majority of associated clinical observed conditions at death were respiratory conditions and respiratory, I would say infections.
Rancourt: Okay Now, these things are not contrary. What we’re saying is there are these primary causes of death. See, when you die, your heart stops eventually. That doesn’t mean that the cause of deaths for everyone who died is heart failure. When you die, the great majority of people in the world have trouble breathing and have a respiratory condition. That doesn’t mean that the primary cause of death is a respiratory infection and so on. You see So we are distinguishing the fact that you can go and say, yeah, there was a respiratory condition here and at what the primary cause of death was. So we are saying that the vaccines, for example, we’re hypothesizing, acted in the following ways to give you this association. One direct toxicity. The onic lipids are toxic, it’s really well known, and the body has a hard time getting rid of them, and they attack tissues and organs and everything.
Rancourt: So toxicity, pure and simple. Second, an over immune reaction, or if you like, an allergic reaction to the injection, that can be a killer. That can kill people. The third one is if you repeatedly inject people with, with a substance, your body in response can tell your immune system, I want you to turn this way down. I want you to suppress yourself because I don’t want an overreaction to this thing that’s coming in routinely into your body. And that mechanism is also really well known. Now, suppression of the immune system in this way is a general suppression of the immune system. So you’re more susceptible to all infections, anything that the immune system can normally defend you against, including cancer, including infections. Okay So we believe that the vaccines are, are having that effect with these multiple doses. So those are the kinds of direct mechanisms that could associate a vaccine rollout to a peak in all cause mortality.
Rancourt: The other thing is, when you’re coming in to roll out the next booster, you’re typically coming in with a team, or another team is coming in with you to test for covid. This is typically a hospital or care home or whatever. Now, when you get a positive test, you’re in trouble. You’re gonna be isolated, you’re gonna be treated aggressively, you’re gonna be given a protocol of treatment that is gonna kill a lot of people, in my opinion. So another mechanism is that temporally, as you’re rolling out the vaccine, you’re also rolling out this medical aggression against people. Yeah. So you’re not, you see, so that’s another way that you would get a temporal association, because we have to explain the temporal association between sudden rollouts and Im, you know, immediate, big, large peaks of excess mortality. The association is undeniable in the data that we see. So the, these are the kinds of, hypotheses that we bring forward to explain these associations.
Jerm: Have you seen any article Sorry, I’ll let you get back onto your, onto your flow. No, no, no. Have you seen any article in the last few years that has actually said these deaths have been caused, we believe, by the vaccine Nothing. Nothing. The vaccines are absolutely magical. They, they are just incredible and amazing, and nothing can go wrong with them.
Rancourt: Yeah, it’s, it’s insane. It’s insane. Even, even the articles where the, the, the scientists who do a thorough study are pretty much forced to admit to themselves that the vaccine killed this person. Let’s say it’s a case study. Sometimes it’s one person. Sometimes they’ve studied five people, whatever. There are case studies out there, and the scientists who are writing these things are so apologetic, they bend over backwards to say that adverse effects are very rare, blah, blah, blah, blah, blah, blah, blah, blah, blah, blah. Yet they present this data that unambiguously shows that the vaccine kill these people, you know, attack their organs directly, and that there’s no way that this young person would’ve died otherwise. And so on. The scientific writing these days has become, it’s embarrassing. It’s almost like you’re living in an ideological religious state, and you cannot say anything that would not be aligned with the ideology.
Rancourt: You know That’s how the scientific writing has become. So in that kind of environment, it’s very difficult to get to the truth. And it’s very difficult to see the amplitude of a phenomenon. And, I don’t suffer from that because, you know, I’ve, I’ve, I’ve always been a rebel, and I’ve always just spoke my mind and looked for the truth and reported the data as I saw it, and put forward the hypotheses that I think make the most sense that I can see, you know And so I have no doubt that of what I advance in, in terms of the hypotheses for the primary causes of death that we’ve seen in the world here until proven otherwise. And I’m open to people bringing counterarguments, but I’m convinced that this was assaults, including the vaccines, is it was horrendous. And I could tell you individual stories of individual countries where it’s just so clear.
Rancourt: You know, you bring in the military people, the lock people in their homes in a, in a Latin American country, and, you isolate the ones that are coughing a bit, and you, you take them away militarily. I mean, the peaks and deaths are out of this world, and they completely coincide with these military campaigns, you know So there is no doubt, in fact the, the big, big main conclusion, there’s two big main conclusions from the paper, and I’ll I’ll tell you them right now. One is that if a pandemic had not been declared, and therefore we had not responded in any way to a declared pandemic, nothing special would’ve occurred in terms of mortality. It would’ve been business as usual. The bacterial infections would’ve been treated as usual. Everything would’ve happened just as usual, and you would’ve had the usual seasonal pattern of deaths with the slight, increase in some countries, because of population is aging.
Rancourt: Everything that normally we would’ve expected would’ve occurred. There would have been no excess all cause mortality during the covid period if we had not had this military campaign that was planned, that is known. So we’re saying, if you hadn’t done this, you wouldn’t have caused the death that you caused the other big conclusion from the paper in comparison to, the nearest historical event that’s similar, but, but very different in many ways, which is 1918. 1918 is very similar in many ways. One of the big differences, it was, it, it was, young adult males and females, but young adults that died in the excess mortality, at least in the United States. Anyone over 50 did not die in 1918 in that, so-called pandemic. So anyway, you analyze all this, and you see the huge correlation with poverty in 1918. You see the respiratory conditions as the main symptom observed on death.
Rancourt: You look at the historic scientific articles that have demonstrated, there are five articles that show in detail from looking at the lung tissue of the people who died back then, that it was a classic bacterial lung infection that killed these people, okay And this is before there was antibiotics. So we recreated the conditions of 1918. We stopped prescribing antibiotics, we stopped treating lung infections, the usual in the classic, usual way. So we recreated those conditions at the same time that we were putting on this huge stress. Now, in 1918, there was huge stress. You had just finished the war. You were just barely recovered from the war. You were recovering your economy. People had to adjust. Young families were suffering terribly, et cetera. people were, were returning from the front with all kinds of conditions. Okay So you had biological stress, extreme biological stress, and you couldn’t treat respiratory conditions.
Rancourt: And in the covid period, same thing. We had all these conditions of imposed biological stress attacks on the body, and you weren’t treating the most common thing, which is lung infections under these conditions, under conditions of stress. Okay So under conditions like that, in the covid period, we’ve quantified that 0.4% of the population was killed, 0.4% in 1918, the best estimate would be about 0.9% of the population. So you have to understand this is, this was a comparable event to 1918 in terms of a huge catastrophe in terms of excess mortality. Those two pandemics lasted about three years, both of them. This is the second big conclusion. When you impose conditions of biological stress like this on a population, you can induce a mortality of 0.1% of the population per year or more. You can reach that level. And in both these cases, 19, 18 and COVID, we were above that level. In other words, just causing huge psychological stress, crash of the economy, locking people down, all everything we did, that kind of thing can kill 0.1% of the population per year, as long as you’re doing it. That’s the other conclusion from our paper. And we believe that that is what has happened.
Jerm: And people don’t think about that. Actually, they forget about it.
Rancourt: Well, people don’t normally think in geopolitical and large scale thinking ways. You know, you, you think about adapting and adjusting to your circumstances and to your life and things you can control, and maybe you get involved in politics. But the kind of work that we’re doing as scientists and thinkers and analysts is to try to understand the phenomenon. The actual phenomenon is bigger than what was happening to individuals. It was structural. It was, you know, led by the US military no less, you know, I mean, this is big. And so to understand it, and, and when you see the, the variety of behaviors in terms of mortality from country to country, jurisdiction, jurisdiction, you, you say, well, okay, there’s a lot going on here. So the answer is not in one specific example. So we show example, many, many countries where nothing, no excess mortality happened until you rolled out a vaccine, and then you get this huge peak that’s immediately coinciding with the rollout of the vaccine.
Rancourt: And so we show graphs and graphs and graphs of many examples like that. We show many examples where you start rolling out the vaccines and you repeatedly roll them out, and then you have continued excess mortality. We show that there are many countries, about 30% of countries that have, I would say, continuing excess mortality beyond the covid period. That’s another phenomenon. Japan, Canada, Germany, and so on. This is striking. And we described that phenomenon in great detail quantitatively in our paper. What is going on there How is it that most countries fall back to zero and these, these countries don’t And they’re in what we call the green cluster in our hierarchical cluster analysis. Those countries tend to be of that type. And they’re countries that tended not to have huge amounts of deaths that were at the beginning until they started rolling out the vaccines, you see
Rancourt: So they didn’t mostly die in those comfortable countries from the structural stress, but they, they are now being killed. And they’re also the countries that, that do the most, injecting it’s booster after booster. And everyone’s proud to get the fifth one and the sixth one, and they just keep doing it, and especially to the elderly. And lo and behold, we have a sustained excess mortality, you know, into 2023 and beyond. So we looked at all of that in this paper as well. It’s a big paper. It’s almost like 10 research articles in one, a
Jerm: Couple comments that I’m sure you get too. And I have been getting them for two years at least, and that is the knee. There was something, I lost my sense of taste for six months, and I’ve never experienced that, right Or there was a bio weapon, it was even in Robert Kennedy’s book, there was a bio weapon. They launched it onto the population, right
Rancourt: Well, let’s do, let, we could do those two things one at a time. So, you know, oh, people were losing their sense of taste. There were these unusual symptoms that you don’t normally see. Well, I’ve been getting correspondence from people around the world. I had one man say my grandfather was an md and he specialized in recording, very unusual symptoms from the flu. And they included loss of taste, loss of smell, loss of, you know, incredible, special headaches, all these other things. He made it his practice to seek those cases out and to document them. I get letters like that. I have personal experience of having had lung infections that were accompanied by unusual symptoms. I once lost my sense of taste for a month. these, these things can happen. You know, what we tend to forget is that there is a large literature of unusual symptoms associated with respiratory conditions, and it’s always been that way just because 90% or more of the time, the, the respiratory infection you get in the winter is routine.
Rancourt: And, you know, you get this series of symptoms and then eventually you recover. Doesn’t mean that when you get a special symptom, oh my God, it must be something very new and very special. It could just mean that your body responds in this way every time you have a lung infection. You don’t know what the population of all the organisms that are playing a role in that. You don’t, you don’t know how they’re interacting, who, what they are, what they’re doing, what else is being affected. If it’s because your immune system was suppressed because of stress, then you don’t know if you have a co-infection in your gut as well. The human body is complicated, and symptoms are unusual. And if the propaganda is saying, oh my God, it’s just unusual, unheard of, and all these symptoms, as soon as you hear of novel symptoms, you are sensitive to them more than you would be.
Rancourt: Or when you hear about them from others, you know Mm-Hmm, like when you’re just getting through, a flu and you know it’s gonna pass, you know you’re gonna recover because it’s your experience and your own life. You don’t make note of every symptom and, and the array and everything. And you, you forget a lot of these things of just how sick you can be. You tend to forget how sick you were certain times when you had these winter infections, right There are times that it lasted a lot longer. There are times when, oh my God, these, these unusual symptoms were, you know, you felt like you had an ear infection as well, and so on and so on. So I would say that you cannot trust these, anecdotal, this anecdotal evidence about those symptoms, even if there are clinical reports about them.
Rancourt: It’s not an epidemiological study to have a clinical report. You know, you’re gonna get it published because that’s what the propaganda is saying. All the journals want to hear about it, and you’ve got case studies that might mention this. It doesn’t mean that it’s representative. So that’s how I respond to the first one, the bio weapon. Well, see, my, my response to that is there are always patents in relation to genomics. They make a lot of money from this. Patents are a racket of, intellectual property where the US imposes its supremacy and can, extract money from other jurisdictions. The patent industry. Now, now it’s being broken because other nations have a high technological advances, and they’re not relying on US patents, and they’re not being intimidated by the US saying, you’re, you’re violating our patent and all this kind of stuff, right But traditionally in the US the patent industry is a scam, and it’s huge.
Rancourt: And so you, you are always, if you’re, the pharma, pharmaceutical industry is always patenting molecules and organisms, and you name it, there are hundreds of patents all the time, every month, because any one of them can become the magic cure for this new thing that they convince people that it now exists, and they, they’ll be able to sell it as the perfect thing that is precisely designed to do this. You know So, patents, the fact that there are patents is meaningless. The fact that there’s a military, laboratories developing bio weapons, that’s also true. And the military’s always developing things, and the military’s always doing research that that is even illegal sometimes, and so on. Or they go to different jurisdictions to do it and so on. That’s just a given. That’s what they do. That’s always happening. But in the end, we can prove that there was, this was not a spreading respiratory condition that caused the excess mortality patterns and their time dependence.
Rancourt: That means that this, any story about this virus is irrelevant to the mortality events that we see, that we observe, that we quantify. It may well be true. They may be developing sequences that they can reproduce in the lab in a Petri dish. I don’t know. but it’s irrelevant to the real world. I would have a call out to the scientist, Jay ey, who has, then some really interesting, arguments that these things cannot reproduce. They, they cannot pandemic. and he’s using, a review of the genomic and scientific literature in relation to that. I think he’s bringing a, a fresh perspective, critical perspective to all of this. A lot would be nonsense, simply generated by career scientists, advancing the main narrative. But, I, I like his perspective. So I don’t know. That’s kind of a partial answer to your second point.
Jerm: I think it’s important because it’s a talking point that dominates, particularly the alternative media, the bio weapon. Bio weapon. I, I would agree that there’s a bio weapon, but I would call it the vaccine.
Rancourt: The vaccine is definitely a military intervention. Mm-Hmm. . And the military definitely wants the capacity to be able to inject things into your body whenever they want, whatever they want. And they, they have the whole, propaganda machine set up so they can, they’re able to do this, and they’re getting people used to the idea that they’re doing this and that you’re a bad person if you don’t agree to be injected, and you’re gonna be fired anyways. So they want the ability to inject the entire entire populations whenever they want, and they would even like to be able to do it in other countries, including China and Russia, right Ultimately. So they want to be able to do this for a couple of reasons. militarily, you can see why they would want to be able to do this. If you can inject whatever you want, you can change people’s health status, you can change, therefore, their ability psychologically to, to resist or to be political.
Rancourt: You can do all kinds of things to people. You can target neighborhoods or areas or populations that you don’t appreciate when you’re injecting everyone. You can send different laws to different places and things like that. So the military, of course, wants to be able to do this. And this was an exercise to, to demonstrate to themselves that they can do it and how they would do it, and what the problems are, and so on. So it’s an experiment. The other thing is, they wanna be able to do it, because they wanna be able to immunize their population or their soldiers or certain other populations, if a pathogen or, a toxic substance that they can have immunity to from, from enemies, okay Or if they wanna do it to their own people, but they wanna protect certain neighborhoods or groups or, or the military and so on, they wanna be able to immunize them.
Rancourt: So injections can be used for that. So there’s all kinds of logical reasons why the military would want this capacity to inject, but what I see as the weapon is the entire structure to inject everybody with whatever they want. That’s the weapon, not the particular substance this time around that was injected into people’s arms. This particular substance was a test of this delivery mechanism using onic lipids fine. And they wanted to fully test that. And in their dream world minds, they can put whatever they want into those nanoparticle capsules. And, you know, this is a great way to go. And they want that technology. But they knew ahead of time that this was not an extremely toxic, product. You know, if people were dying coming out of the injection room, it would’ve, it would’ve ended really quick, you know, if they were dropping dead, even the few that were having immediate problems, the, the, the viral videos were giving them a hard time.
Rancourt: Were given the establishment a hard time. You see, it needed to be toxic enough that there are adverse effects. It needed to be real. It couldn’t just be saline solution had to be real, otherwise, you, you wouldn’t be able to hide it. The the fact that you’re, it’s an entire scam. And adverse effects actually help you because it proves that it’s a real product. You know, every medication has a risk. They’ve been driving this home to us. And so you accept that there’s a risk when you’re being helped by the government, and this is proof that, that you’re being helped the fact that there are adverse effects. So all of this kind of fits together in their scheme. My own personal view is that this particular injection was not any kind of special bio weapon or anything like that.
Jerm: It’s very important to me that you have a few times in this conversation dropped in the military or the Department of Defense. It’s a conversation that I’ve been having, and very few others are engaging in. They keep focusing on Fauci and on the WHO, and they’re mostly just frontmen. They’re pawns. This is effectively a military operation that, that we experienced. Oh,
Rancourt: Yeah. It’s structural, it’s huge. It’s institutional. It’s an, the entire military intelligence complex was running this thing. And they control the propaganda and they control the internet. They control everything. They are the ones who structured this. And you have to understand that Western US led propagandas extremely powerful. It penetrates into China and Russia, you know, fairly easily. It, it penetrates. And this is a case where they’re using human health, and so they’re tying into the natural fear that people have about pathogens and being exposed to something. And, and you know, how you’re always looking out for, not putting yourself in danger. It exploits that. And so if you’ve got propaganda that penetrates, and it exploits that, that means that Russia and China, for example, are vulnerable to what you’re doing, because their own populations will scream bloody murder if they’re not providing the same protection with a vaccine, okay
Rancourt: Or if they’re not locking down, or if they’re not doing this and that. So it’s not the fact that Russian, China were doing essentially the same thing, does not mean that they’re controlled by the same forces that control the us. I don’t accept that in that notion. It simply means that they also want militarily the ability to do this, and they need to placate their own populations. They need, they need to show that their team players, when there’s a global pandemic, you know, there’s an image thing that is very important as well. And you can look at the chronology of when influential papers came out in the leading journals blaming China, that happened before China started showing films of building hospitals and locking down, okay And they were explicitly blaming China and saying that China had not locked down quickly enough and that kind of thing.
Rancourt: And we we’re gonna have, be the, those responsible for causing millions of deaths, right China’s very sensitive to that, especially in an era of outright open economic war with the United States. If in addition you can say that they were, they’re so irresponsible that they’re the reason that millions of people around the world are dying, you know, it makes it easier to attack them in more ways economically, which then harms the world economy to the point where people in the west are suffering, but they accept it because you have to attack China because they’re so nasty. You know, this kind of thing. Mm-Hmm. So it all kind of fits together that way. I think those are just my geopolitical views on the situation.
Jerm: The thing is though, Danni geopolitical views in relation to covid are interlinked. That’s, that’s the reality.
Rancourt: Oh, absolutely. There’s no doubt about it. The campaigning, the institutional structures, the, the, they were not hiding it. It, it’s all, it’s all documented. They’re hiding only the most sensitive parts. So the parts that they don’t want you to see, but when they have to involve most scientists, most institutions, and then they’re, they do it in a public forum type of atmosphere. They indoctrinate these people basically, and they get them used to doing this. They manipulate. And so all of that is visible. It’s known, but clearly this was a, a military campaign.
Jerm: You’ve covered quite a lot of territory. So if you don’t mind, for the purposes of a soundbite, would you mind summarizing what you’ve spoken about So basically, you looked at about, what did you say, 125 countries. We’ve
Rancourt: Just put out what is arguably the largest study of its kind, using hard data, which is all cause mortality as a function of time. We’ve looked at the spatial temporal variation of that mortality across the covid period. And we are using sophisticated statistical analysis methods, and we’re demonstrating a few basic really fundamental things. One is that this was not a viral respiratory pandemic. There was no pandemic in that sense. Two is that it was a period of huge excess deaths comparable to 1918. Those excess deaths are highly variable from country to country, because different countries were doing different things, which all amount to biological stress, eventually being the primary cause of death, and also, aggressive, medical interventions. Okay But those are the ways that you are killing people. And, and I include vaccines in there. We have demonstrated a complete understanding of all cause mortality, excess mortality during the covid period as a consequence of those kinds of assaults. I think those hypotheses are highly valid, and I, I look forward to being disproved on these points if possible. What this means is that if you assault entire civilizations, entire societies in this way, you will cause mortality at the rate of at least more than 0.1% of the population that will die every year, that you continue to make these assaults. And so that’s the number that comes out from looking at 1918 in the Covid period. And it has nothing to do with, as a primary agent, a viral respiratory pandemic.
Jerm: Now, I know that you are also fairly awake with regards to, as you’ve pointed out, the geopolitical scenarios and that sort of thing. What do you think is going to unfold in the next few years Do you think they’re going to attempt another operation like this Or do you think we, , we, we made it through it I
Rancourt: Think they’ll decide as they go. They will test things. They will attempt things. They will decide when it would be useful to do it or not. Do it, do it again, or do do it in certain places. They’re very, flexible and they adapt quickly. And this is a time of war. You have to realize, the US has decided to try and destroy the rapid advances of Russia and China, and they’re very aggressively doing, economic blo blockades and financial blockades. And, they’re building up militarily to, do these blockades. They’re actually at war in a hot war in Ukraine right now as a proxy state to try and hurt Russia. This is a very violent and very aggressive period in our, in world history. and I’m not even mentioning, or I haven’t yet mentioned Gaza, Israel, Yemen, Lebanon, you name it, you know, the, the, the Middle East is yet another huge hotspot.
Rancourt: Mm-hmm, , where the US is very much involved and has traditionally been the boss, via, via its collaboration with, and its funding of Israel. We’re in a very dangerous place because these, warring times are happening at the same time that the USA is coming down a notch. As the world leader, the elite that control the US don’t want to have anything to do with this new world that would be multipolar. They want to do whatever they can to enrich themselves through war to the limit if they have to. They would rather destroy many things and then rebuild and be in control after that. So there’s a lot of crazy thought going on. A lot of criminality in the minds of these, of these people. Those are the circumstances in which we’re living, and that’s way more important than whether or not they’re going to have repeat exactly the same, scam on western populations and so on.
Rancourt: So geopolitical changes and factors and geo-economic factors are going to affect our lives way more than whether or not Fauci or someone else decides to do this kind of thing. These are big, big changes, and there is going to be a massive ratcheting down of the US economy, and that is going to have a huge impact on the US middle class. There’s going to be unrest as a result of that. there’s already a class war in the US between the working class, traditionally the middle class, and, the, the, the, the elite and the managerial class and the professional class who are completely on side with the globalist project of war and of destruction instead of cohabitation with these other powerful emerging nations. They don’t want development of Africa and Latin America. Latin America is a region of exploitation for the US and they want to keep it that way.
Rancourt: So there’s some big changes ahead, and we’re going to see them in the next one and two decades from the start, I have said, you’re not gonna understand what’s happening to us until you’ve seen it for the next decade. You know, it’s gonna take a decade before you can really see where this was all going. The only thing that’s keeping the US a little bit sane and within certain bounds is that China and Russia and others are developing independence and strength, military and economic, okay And they’re, aligning themselves with other powerful players, including Iran. There’s a resistance mounting the bricks, nations, the security alliances. They’re tired of being pushed around and being intimidated by, sanctions and financial, coercion and this kind of thing. And so that pushback to the degree that it’s successful is what’s going to prevent wars basically manipulated and, and made and fabricated and run by the USA because they make a lot of money from these wars.
Rancourt: So that’s what’s going to kind of slow things down. And hopefully some people in the US will decide that it might be better to have a more stable democratic society with a structured hierarchy and allow a middle class and so on, and have peace within the society and coexist and cooperate globally with other players rather than try to just dominate everything. But the only thing that will actually bring that shift is strength in Russia, China, and other places. And, and the developing, world coming, coming into its own, including Africa. Some remarkable things happening in Africa right now. Basically
Jerm: What you’re saying is that, as we head towards Mordor, the fellowship becomes all the more important
Rancourt: Yes. Fellowship and the big players recognize that there’s so much cohesion being created and encouraged among the people who want to resist this continued dominance of the us.
Jerm: How can I keep up with your work
Rancourt: Regarding the Covid research and the big reports I think the best place is the, correlation website. So correlation-canada.org, all the research is there. There’s a covid section, you can look at it and so on. And then there’s, my own website where I try to put everything there in the different, research areas and everything. So that’s all one word.
that has my research in, climate, covid, medicine, social theory, political theory, and all the areas of science that I worked in as well that has, you know, a lot of stuff there. My, my own personal website and I’m on X Twitter if you like. and I’m on Substack now and I’m really enjoying the Substack experience. So there you go. I mean, people can find me. My, just use my name and do some searching and you’ll find it right away.
Jerm: Deni, thank you for joining me in the trenches.
Rancourt: It was a great pleasure. I was happy to be here.
—End Transcript—-
Jerm Warfare Introduction
Anyone who has followed my work since 2020 knows about Denis Rancourt and our numerous conversations about COVID-19 and climate change.
But especially COVID-19.
Or rather, COVID-1984 (to borrow from Hrvoje Morić).
I recommend listening to his conversation about all-cause mortality data across several countries, showing no evidence of a pandemic, and his conversation about vaccine-related deaths in the Southern Hemisphere. (Plot twist: the jab was neither safe nor effective.)
The following conversation, however, is the crème de la crème. Denis and his colleagues have published their most extensive paper to date, analysing all-cause mortality across 125 countries throughout the entire alleged COVID-19 pandemic.
We already know the conclusion (that there was no pandemic), but the scientific journey is the fascinating part.
The duration of the ‘pandemic’—2020 to 2023—is based on the declaration made by the WHO. (Speaking of the WHO, make sure to listen to my conversation with WHO insider Astrid Stuckelberger.)
The Art of Liberty Foundation – Important News is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Subscribed
The paper in question, Spatiotemporal variation of excess all-cause mortality in the world (125 countries) during the Covid period 2020-2023 regarding socio economic factors and public-health and medical interventions, is over 500 pages and has a really long title.

They analysed all-cause mortality data from 125 countries, covering about 35% of the global population.
What they found is an excess mortality rate of 0.392% during 2020-2022, compared to 0.97% during the 1918 Spanish Flu.
Interesting.
India, not included in this study, had an excess death rate of 0.26% in 2021 alone.
The paper projected 30.9 million excess deaths globally from 2020-2022, with 16.9 million deaths related to the rollout to the jab.
Denis noted that the large variations in mortality rates were inconsistent with a viral outbreak. Clustering, which is not typical of viral behaviour, was apparently observed. Put another way, if a so-called virus spreads through a population, there shouldn’t be pockets of sick—or dead—people.
Now what?
What was the cause of excess mortality, in that case?

Denis covered what was in the paper and touched on the geopolitical link between the COVID™ era, wars, climate change and the sinking Western empire.
About Dr. Denis Rancourt
Dr. Denis Rancourt is a scientist and social theorist and is currently a researcher at Ontario Civil Liberties Association (ocla.ca), since 2014. He holds B.Sc.(1980), M.Sc (1981). and Ph.D. (1984, University of Toronto) university degrees in physics.
He has been a Natural Sciences and Engineering Research Council (NSERC) of Canada international post-doctoral candidate in prestigious research laboratories in both France and The Netherlands (1984-85, 1985-86).
He became a national NSERC University Research Fellow, in Canada. He was a professor of physics at the University of Ottawa for 23 years, attaining the highest academic rank of tenured Full Professor.
He developed new courses and taught over 2000 university students, at all levels, and in three different faculties (Science, Engineering, and Arts).
He supervised more than 80 junior research terms or degrees at all levels from post-doctoral fellow to graduate students to NSERC undergraduate researchers. Several of his former graduate students are government and private-sector scientists, university professors, teachers, managers, and business leaders.
He headed an internationally recognized interdisciplinary research laboratory, and attracted significant research funding for two decades.
Dr. Rancourt has been an invited plenary, keynote, or special session speaker at major scientific conferences 41 times, including recently in 2020 and 2021 (by virtual attendance). He has published over 100 research papers in leading peer-reviewed scientific journals, in the areas of physics, chemistry, geology, materials science, soil science, and environmental science.
He has made fundamental scientific discoveries in the areas of environmental science, measurement science, soil science, bio-geochemistry, theoretical physics, alloy physics, magnetism, and planetary science.
Dr. Rancourt’s scientific impact factors (h-index) is 41, and his articles have been cited almost 6,000 times in peer-reviewed scientific journals.
Dr. Rancourt is a frequent media commentator. His medical, political and social theory articles and interviews are published in many venues. His recent video interviews and reporting videos about the science of the COVID-19 epidemic and the science of face masks for preventing viral respiratory diseases have been viewed more than 2 million times, in both French and English.
About Jeremy “Jerm” Nell
Jerm is a South African cartoonist whose work has appeared in a bunch of publications, online and offline, such as the Sunday Times, The Star, City Press, Rapport, Beeld, The Times, FHM, Playboy, Rolling Stone, TIME, Daily Maverick, The New Age, Cosmopolitan, EWN and others. His work has also appeared in Belgian, Spanish, Dutch, and Indian publications. His editorial cartoons now appear in Eyewitness News. https://jermwarfare.com
AboutAbout the Author

Etienne de la Boetie2 is the founder of the Art of Liberty Foundation, the author of “Government” – The Biggest Scam in History… Exposed! and the editor of the Art of Liberty Daily News on Substack and Five Meme Friday, which delivers hard-hitting voluntaryist memes and the best of the alternative media.
He is the author of The Covid-19 Suspects and Their Ties to Eugenics and Population Control/Reduction and Solving Covid – The Covid 19, Eugenics, and Vaccine/Drug Scam Timeline

A start-up public policy organization: Voluntaryist crime fighters exposing inter-generational organized crime’s control of the “government,” media and academia. The foundation is the publisher of “Government” – The Biggest Scam in History… Exposed!– How Inter-Generational Organized Crime Runs the “Government,” Media and Academia.
We publish The Daily News, a free survey of the best of the alternative media, censored videos, and documentaries, and the Daily News Digest, a once-per-day-summary of the Daily News as a premium service for paid subscribers of any Art of Liberty Foundation Substack and Five Meme Friday – a free weekly e-mail or Telegram summary of the best of the alternative media, censored truth videos, and at least five hot, fresh, dank liberty memes every week, and “Government,” Media, and Academia Exposed! – A Telegram summary of the best mainstream and alternative news stories proving our thesis that all three are being hierarchically controlled by inter-generational organized crime interests. You can read our 2023 Annual Report here.
Go paid at the $5 a month level, and we will send you both the PDF and e-Pub versions of “Government” – The Biggest Scam in History… Exposed! and a coupon code for 10% off anything in the Government-Scam.com/Store.
Go paid at the $50 a year level, and we will send you a free paperback edition of Etienne’s book “Government” – The Biggest Scam in History… Exposed! OR a 64GB Liberator flash drive if you live in the US. If you are international, we will give you a $10 credit towards shipping if you agree to pay the remainder.
Support us at the $250 Founding Member Level and get a signed high-resolution hardcover of “Government” + Liberator flash drive + Larken Rose’s The Most Dangerous Superstition + Art of Liberty Foundation Stickers delivered anywhere in the world. Our only option for signed copies besides catching Etienne @ an event.